Aging in place means staying in your own home as you get older — but making it work safely takes planning. Here’s everything you need to know before deciding.

Aging in place means staying in your own home as you get older — rather than moving to an assisted living facility, a nursing home, or a family member’s house — even as your physical or cognitive needs change over time.
It’s what the vast majority of older adults say they want. Surveys consistently show that more than 75 percent of adults over 50 want to stay in their own home for as long as possible. The gap between what people want and what actually happens is almost entirely explained by one thing: preparation. People who plan for aging in place succeed at it. People who assume it will work out without planning are the ones who end up making rushed decisions after a crisis.
This guide covers what aging in place actually means in practice, what makes it work, what makes it fail, and how to assess honestly whether it’s the right choice for your specific situation.
Check out our FREE aging in place checklist here!
What Aging in Place Actually Means
Aging in place doesn’t mean living exactly the way you live now, indefinitely, without any changes. That’s not what it means and expecting it to work that way is the most common planning mistake people make.
What it actually means is living in your own home with whatever combination of modifications, support services, and technology allows you to do so safely and comfortably as your needs evolve. The home changes. The support system changes. The person changes. The goal — staying in a familiar, chosen environment rather than an institutional one — stays the same.
For some people aging in place means grab bars in the bathroom and a walking cane. For others it means significant home modifications, daily in-home care, and a full suite of monitoring technology. The right version of aging in place is the one that matches your actual situation — not an idealized version that ignores real physical or cognitive changes.


Why Most People Want to Age in Place
The preference for home over institutional care isn’t just sentiment — it’s backed by real, documented benefits that affect both quality of life and health outcomes.
Familiarity and Comfort
A home lived in for decades is a deeply familiar environment — spatially, emotionally, and cognitively. The layout is automatic. The neighborhood is known. The routines are embedded. For older adults, and particularly for those with early cognitive changes, familiar environments support independence and orientation in ways that new environments — however well-designed — simply can’t replicate quickly.
Control and Autonomy
Staying at home means staying in control of your own daily life — when you wake up, what you eat, who visits, how you spend your time. This autonomy is not a luxury. Research consistently shows that perceived control over one’s environment is a significant predictor of both physical health and cognitive function in older adults. Loss of that control — even in a high-quality care setting — is associated with measurable declines.
Social Connections
Home is where existing social networks live — neighbors, friends, community organizations, familiar local businesses. Moving, even to a setting designed for social engagement, severs those connections and requires building new ones at an age when that’s significantly harder. Social isolation is one of the most significant risk factors for cognitive decline and physical health deterioration in older adults. Aging in place protects existing social connections rather than starting from scratch.
Better Health Outcomes
Studies comparing health outcomes for older adults who age in place versus those who move to institutional care — controlling for health status — consistently show better outcomes for those who remain at home with appropriate support. The combination of familiar environment, maintained autonomy, and preserved social connections produces measurable health benefits that aren’t fully replicable in institutional settings.
Cost
Assisted living facilities cost an average of $4,500 to $6,000 per month nationally. Nursing homes cost significantly more. Aging in place — even with home modifications, in-home support services, and monitoring technology — is typically substantially less expensive for most people at most stages of the aging process. The cost comparison shifts at very high levels of care need, but for most older adults aging in place is the more affordable option as well as the preferred one.

What Makes Aging in Place Work
Successful aging in place is built on four foundations. People who have all four in place succeed. Those who are missing one or more encounter preventable problems.
A Safe and Modified Home Environment
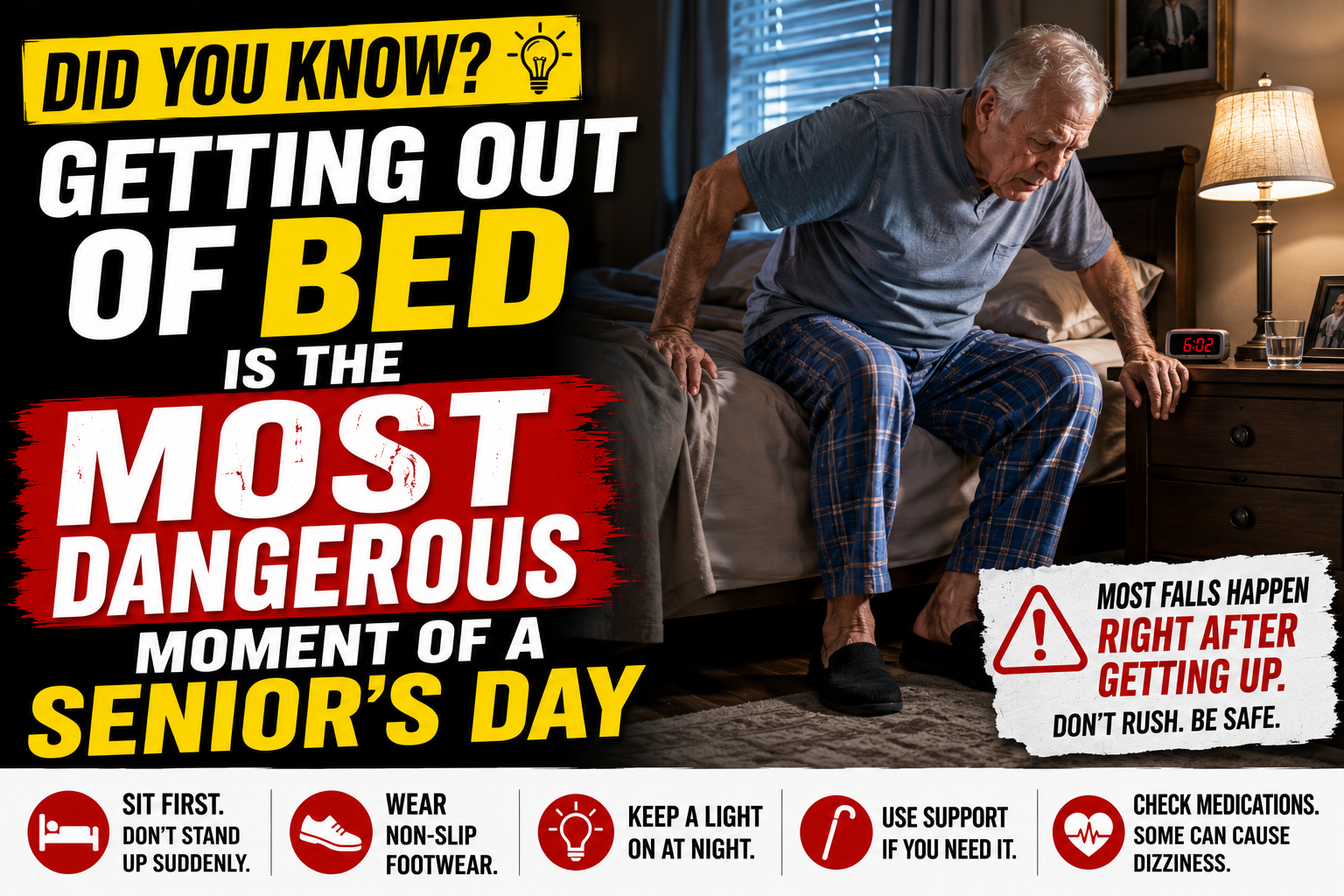
The home needs to be modified to match changing physical needs rather than assuming the person will adapt to a home designed for someone younger and more physically capable. The most critical modifications are bathroom safety — grab bars, non-slip surfaces, shower seating — and fall prevention throughout the home.
Our guide on how to make your home safer as you age covers the complete modification picture. Our home safety checklist gives you a systematic room-by-room assessment tool. The specific products that make the biggest difference — grab bars, shower chair, non-slip bath mat, bed rail, toilet safety rails — are all covered in dedicated reviews.
A Support Network
Aging in place doesn’t mean aging alone. The most successful aging in place situations involve a combination of formal and informal support — family members who check in regularly, neighbors who are aware and involved, and professional services that fill the gaps formal support can’t cover.

Building and maintaining that support network proactively — before a crisis makes it urgent — is one of the most important aging in place planning steps. This means having explicit conversations with family members about roles and responsibilities, building relationships with neighbors, and identifying the community resources available before they’re needed rather than searching for them under pressure.
Appropriate Technology
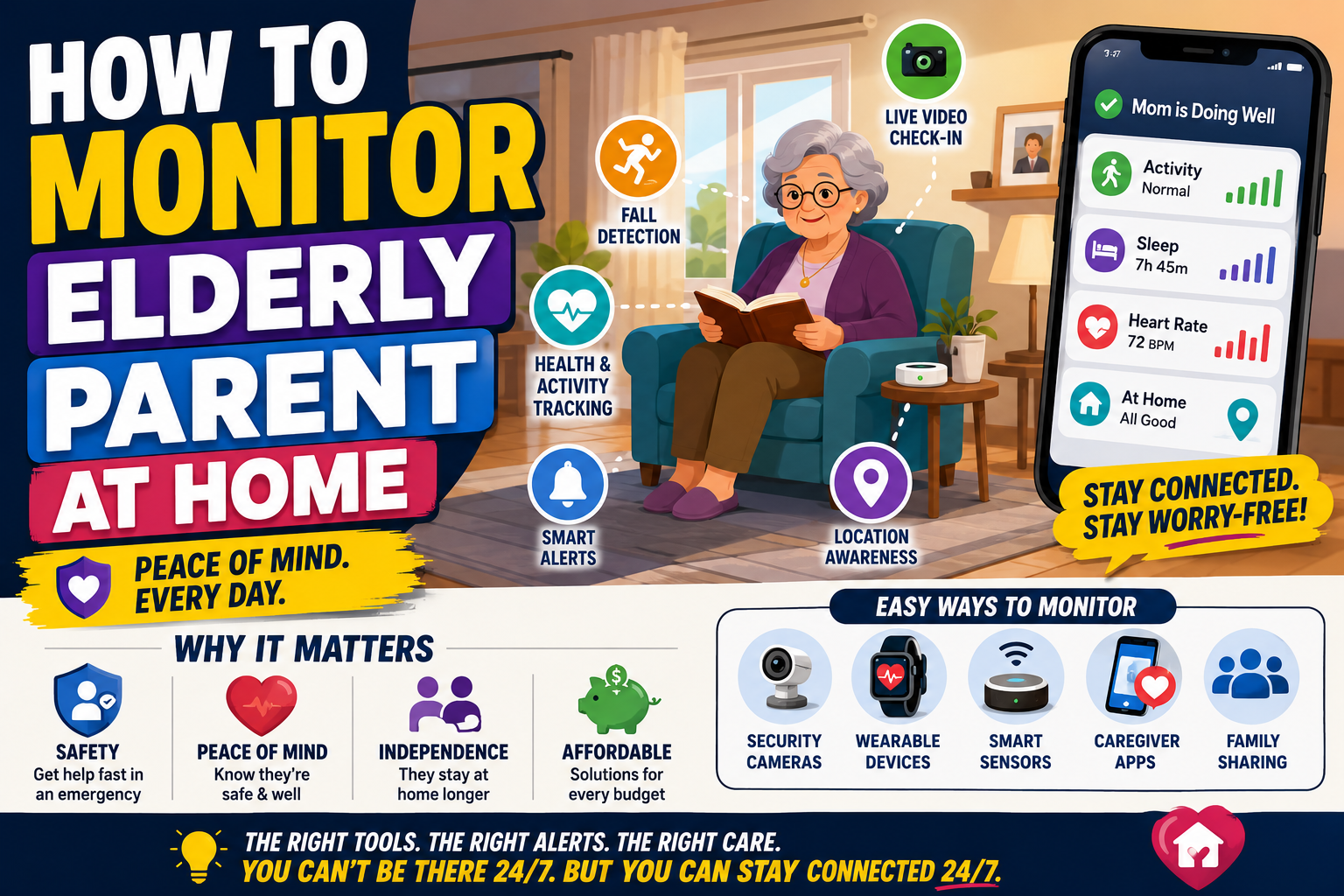
Technology has dramatically expanded what’s possible for aging in place over the last decade. Medical alert devices with automatic fall detection provide safety coverage when no one is physically present. GPS tracking provides location awareness for active seniors and those with memory concerns. Smart home technology — voice-controlled lights, smart locks, video doorbells — reduces the physical demands of daily tasks and keeps people connected without requiring them to navigate complex interfaces.
The SecuLife Smartwatch is one of the most comprehensive single-device solutions for aging in place safety — combining fall detection, GPS tracking, SOS calling, and two-way communication in a wrist device that doesn’t require a smartphone or technical management from the wearer. Our full SecuLife review covers everything you need to know.
→ See the SecuLife Smartwatch on Amazon
Proactive Health Management
Aging in place works best when health conditions are actively managed rather than reactively treated. Regular medical appointments, medication reviews specifically focused on fall risk and functional side effects, vision and hearing checks, and physical therapy for specific functional limitations all contribute to maintaining the physical capacity that makes independent living sustainable.
Preventive health management costs significantly less than the emergency care that follows from unmanaged conditions — and keeps the functional capacity that makes aging in place viable for much longer.
What Makes Aging in Place Fail
Understanding the common failure points helps avoid them. Most aging in place failures follow one of several predictable patterns.
Waiting for a Crisis to Plan
The most common pattern: everything is fine, planning feels unnecessary, then a fall or medical event creates a sudden urgent need for major changes. Decisions made under crisis pressure — often by multiple family members with different perspectives, with limited time and information — are rarely the best decisions. The people who age in place most successfully made their plans before anything went wrong.
Underestimating the Home Modification Requirement
A standard home built for a healthy younger adult is not designed for aging in place. Bathrooms without grab bars, bedrooms with high beds, stairs between floors, and poor lighting are all hazards that become progressively more dangerous as physical capacity changes. Many people underestimate both how much modification is needed and how much difference those modifications make.
Isolation
Aging in place without adequate social connection and support is genuinely dangerous — not just unpleasant. Social isolation is associated with accelerated cognitive decline, depression, reduced physical activity, and delayed recognition of health changes that warrant medical attention. Aging in place plans that don’t explicitly address social connection and support are incomplete.
Caregiver Burnout
When aging in place depends primarily on one family caregiver — typically a spouse or adult child — caregiver burnout becomes a genuine risk that can end the arrangement as surely as any health event. Sustainable aging in place plans distribute caregiving responsibility and include formal support services rather than relying on one person indefinitely.
Cognitive Decline Without Planning
Mild cognitive impairment and early dementia are compatible with aging in place for most people — with appropriate modifications and support. Moderate to advanced dementia typically requires either significant in-home care or a care setting change. Planning for this progression — knowing what the triggers for a care setting change will be, having that conversation before cognitive capacity is lost — is a critical part of aging in place planning for anyone with dementia risk.
Our guides on home safety for seniors with dementia and wandering prevention for dementia cover the specific modifications needed as cognitive changes emerge.



Is Aging in Place Right for You?
The honest answer to this question is different for different people and at different points in time. Here’s a framework for assessing it honestly.
Factors That Support Aging in Place
- Your home is a single story or the primary living areas are on one floor
- You have family or friends nearby who are available and willing to be part of a support network
- Your health conditions are stable and actively managed
- You’re willing to make home modifications and use assistive technology
- Your community has accessible services — grocery delivery, transportation, healthcare
- You have adequate financial resources for modifications and support services
- You are socially connected and have meaningful activity in your life
Factors That Complicate Aging in Place
- Multi-story home with primary rooms on different floors and no elevator
- Isolated location with limited access to services
- Limited or distant family support network
- Significant cognitive decline without adequate in-home support
- Health conditions requiring daily medical care that can’t be arranged at home
- Social isolation with no community connections
- Financial limitations that prevent necessary modifications or support services
None of the complicating factors are automatic disqualifiers — all of them can be addressed to varying degrees with planning, resources, and creativity. They’re factors to weigh honestly rather than reasons to give up on the goal.
Questions Worth Asking Yourself
Beyond the checklist, a few honest questions help clarify whether aging in place is workable for your specific situation:
- If I fell at home and couldn’t get up, what would happen? How long would it be before someone knew?
- Is my home physically set up to support independent living as my mobility changes, or would significant changes be required?
- Do I have people in my life who could provide support if I needed it — and have I had explicit conversations with them about what that might look like?
- Am I managing my health proactively, or reacting to problems as they emerge?
- Am I socially connected in ways that would continue if I couldn’t drive or leave the house easily?
Honest answers to these questions — not optimistic assumptions — are the foundation of a realistic aging in place plan. Our guide on warning signs you may not be safe living alone covers the specific signals worth monitoring over time.

Aging in Place vs. Assisted Living — Honest Comparison
For many families this is the core decision — age in place or move to a care setting. Here’s the honest comparison across the factors that matter most.
Cost
Aging in place is typically less expensive than assisted living at equivalent care levels. The comparison shifts as care needs increase — very high levels of in-home care can approach or exceed assisted living costs. The specific numbers depend heavily on location and care needs.
Safety
Neither option is automatically safer. A well-modified home with appropriate technology and support is genuinely safe for most older adults. An assisted living facility provides more immediate human supervision but introduces its own risks — medication errors, falls in unfamiliar environments, infections. Safety depends on the quality of implementation in either setting.
Quality of Life
Research consistently favors aging in place for quality of life — autonomy, familiar environment, maintained social connections, and sense of control all score higher for people living at home than in institutional settings. High-quality assisted living narrows this gap but rarely closes it for people who strongly prefer home.
When Assisted Living Becomes the Right Choice
Aging in place becomes genuinely untenable — rather than just more difficult — when care needs exceed what can realistically be arranged at home, when cognitive decline is severe enough that unsupervised home living creates unmanageable safety risk, or when the primary caregiver can no longer safely continue. Knowing these thresholds in advance and having the conversation before they’re reached is worth doing now regardless of current health status.
Starting Your Aging in Place Plan
The best time to start planning for aging in place is before you need to. Here’s where to begin.
Assess your home. Walk through it with fresh eyes — or have a Certified Aging-in-Place Specialist (CAPS) do a professional assessment — and identify what needs to change. Our home safety checklist is a practical starting point for self-assessment.
Address the highest-impact modifications first. Bathroom safety — grab bars, non-slip surfaces, shower seating — is the most important starting point for almost everyone. Our complete guide on how to make a bathroom safer covers every upgrade worth making.
Put a safety net in place. A medical alert device with automatic fall detection ensures that if something happens at home, help is called immediately. For anyone planning to age in place this is a non-optional component of a complete safety plan. Our guide on signs it’s time for a medical alert system helps assess when to start and our guide on how much a medical alert system costs covers the financial picture clearly.
Build your support network explicitly. Have the conversations with family members, neighbors, and friends about what support might look like — before you need it. Vague assumptions about who will help are not a support network.
Review your health management. Request a medication review focused on fall risk and functional side effects. Get your vision and hearing checked. Ask for a physical therapy referral for any specific functional limitations worth addressing.

Frequently Asked Questions
How much does aging in place cost?
The cost varies enormously based on the level of modification and support needed. Basic home modifications — grab bars, non-slip surfaces, a bed rail, improved lighting — typically cost $500 to $2,000. More significant modifications like ramps, walk-in showers, or stair lifts cost more. In-home care services range from $25 to $35 per hour nationally for home health aide services. A medical alert device adds $20 to $50 per month. The total is highly individual — but for most people at most stages of aging, aging in place remains less expensive than assisted living alternatives.
Can I age in place if I live alone?
Yes — millions of people live alone and age in place successfully. Living alone makes the support network and safety technology components of the plan more important rather than impossible. A medical alert device with automatic fall detection is particularly critical for anyone living alone. Regular check-ins from family or friends, relationships with neighbors, and community service connections all provide the support network that replaces the built-in safety of shared living.
What home modifications are most important for aging in place?
Bathroom modifications have the highest impact — grab bars at the shower and toilet, non-slip surfaces, and shower seating address the highest-risk room in the home. After the bathroom, bedroom safety modifications — bed rail, adequate lighting, clear path to bathroom — and stair safety modifications — handrails on both sides, non-slip treads, adequate lighting — address the next highest risk areas. Our complete guide on how to make your home safer as you age covers the full priority order.
At what point does aging in place become unsafe?
Aging in place becomes genuinely unsafe — rather than just more challenging — when care needs can’t be safely met at home, when cognitive decline is severe enough that unsupervised living creates consistent safety emergencies, or when the support network has collapsed. The warning signs to watch for are covered in our guide on warning signs you may not be safe living alone. Most people reach those thresholds later than they expect when aging in place is actively planned rather than assumed.
Does Medicare cover aging in place services?
Medicare covers some home health services — skilled nursing care, physical therapy, occupational therapy — when medically necessary and ordered by a physician. It does not cover custodial care like help with bathing, dressing, and meal preparation unless combined with skilled care. Medicare Advantage plans vary in what home-based services they cover — check your specific plan. Medicaid waiver programs in many states cover significant home and community-based services for eligible individuals. Local Area Agencies on Aging are a valuable resource for identifying what’s available in your area.


Your Home. Your Terms. Your Timeline.
Aging in place is not a passive choice — it’s an active one that requires planning, modification, and honest ongoing assessment. The people who do it successfully aren’t those who simply decide they want to stay home. They’re the ones who build the foundations that make staying home safe and sustainable.
Those foundations — a safe home environment, a support network, appropriate technology, and proactive health management — are all within reach for most people at most stages of aging. The earlier they’re put in place the longer they sustain the goal of staying home on your own terms.
Start with your home assessment this week. Address the bathroom first. Put the safety net in place. Build from there.
→ Get the SecuLife Smartwatch on Amazon — the safety net every aging in place plan needs

About the Author
Carol Simmons is a Certified Aging-in-Place Specialist (CAPS) who spent 15 years helping people plan and implement aging in place across Florida and the Southeast. She has seen what works, what doesn’t, and what separates the people who successfully age in place for decades from those whose plans fall apart at the first serious challenge. She writes for Elder Safety Guide to give people the honest, practical guidance that makes the difference between a plan that works and one that doesn’t.