Half of older adults who break a hip never return to the home they lived in before the fracture.
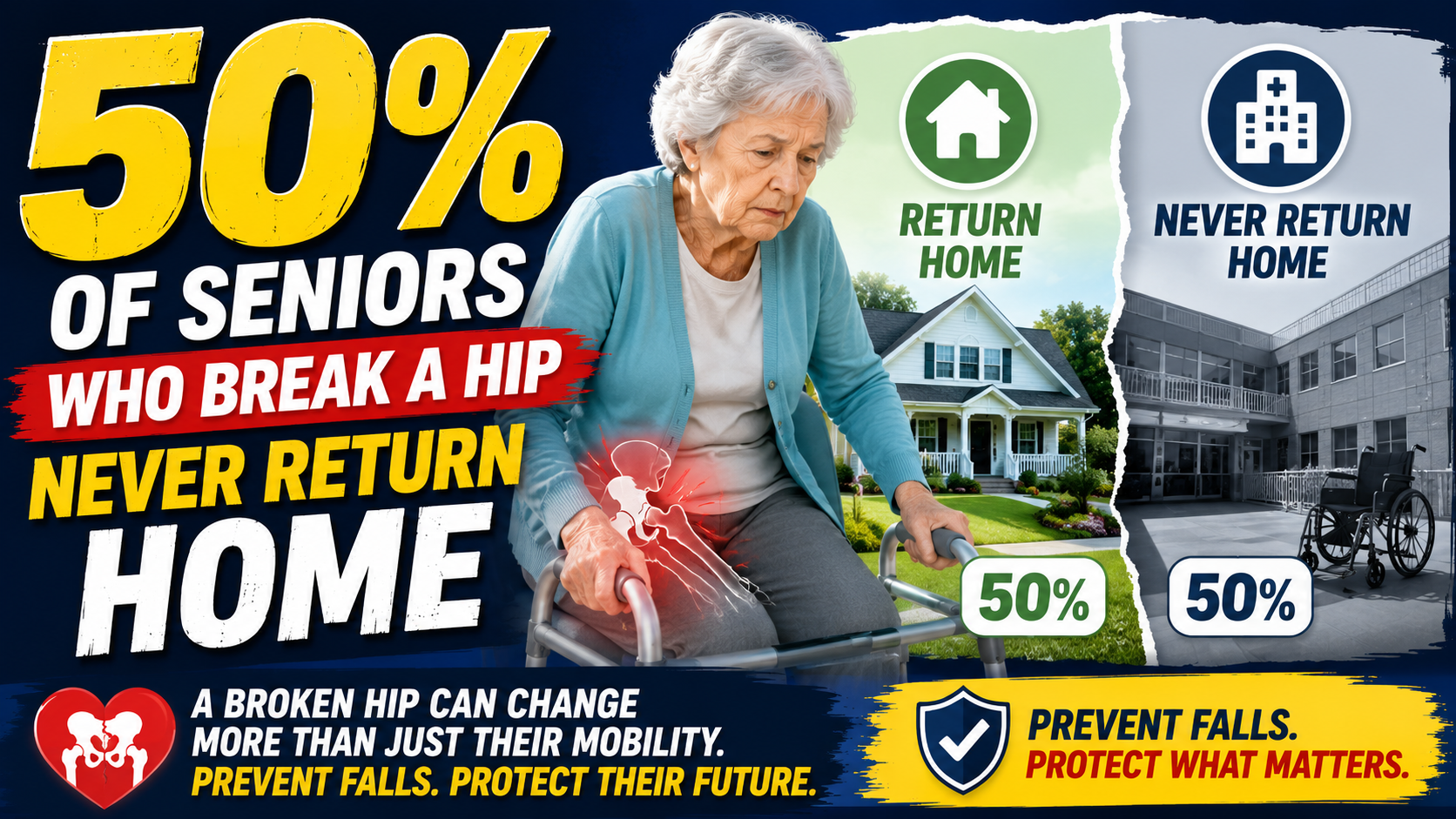
Not the majority. Not most. Half. Fifty percent of people who were living in their own homes — managing their own lives, maintaining their independence — before a hip fracture do not return to that home afterward. They move to assisted living. To a family member’s home. To a nursing facility. To a level of care that the fracture made necessary in ways that independent living could no longer accommodate.
This is one of the most consequential statistics in senior health. And most families don’t know it until a hip fracture has already happened.
What Happens After a Hip Fracture
Understanding why half of hip fracture patients don’t return home requires understanding what a hip fracture actually does to an older adult — not just the bone, but the cascade that follows.
As covered in our complete guide on hip fractures kill 1 in 4 seniors within a year — the fracture itself is the beginning of the problem, not the whole of it. Surgery. Immobility during recovery. Rapid muscle loss that occurs during even brief periods of reduced activity in older adults. The pneumonia risk that accumulates during immobile recovery. The delirium that follows anesthesia and hospitalization in a proportion of older adults and that leaves lasting cognitive changes.
The hip fracture that occurred in a few seconds produces a recovery period measured in months — during which the physiological reserves that supported independent living before the fracture are depleted. Many older adults who were managing independently before the fracture emerge from recovery with functional capacity that has fallen below the threshold independent living requires.

This is how half of hip fracture patients don’t go home. Not because of a single dramatic decline but because the recovery process itself — necessary, appropriate, well-managed — consumes reserves that weren’t fully there to begin with.


The One-Year Mortality — The Other Half of the Statistic
The 50 percent figure for not returning home is striking. The mortality figure alongside it is starker. Approximately one in four older adults who sustains a hip fracture dies within 12 months.
Put together: of every four older adults who break a hip, one dies within a year, and one to two more don’t return to independent living. Only one or two of the four return to something close to their pre-fracture life.
These numbers don’t represent inevitable outcomes. They represent the current state of outcomes — what happens when falls occur in homes that haven’t been modified, when falls go undetected for hours, when the recovery process isn’t optimally managed. Each of those variables is changeable. The statistics change when the variables do.


The Fall That Causes a Hip Fracture — What It Looks Like
The fall that causes a hip fracture is usually indistinguishable from the falls that came before it. Same floor. Same time of day. Same movement pattern. Until it isn’t.
This is the most important thing to understand about hip fracture prevention: the fall that produces a fracture is not a special fall. It’s a fall that landed differently, at a slightly different angle, with bone density that had reached the threshold where that landing produced a fracture rather than a bruise.
As covered in our guide on the warning sign families miss until it’s too late — the fall that changes everything is almost always preceded by falls that didn’t. The pattern was there. The signal was there. The response that would have made the difference — home modifications, fall detection technology, medication review, balance exercise — was possible before the hip fracture made it irrelevant for that particular fall.
What Reduces Hip Fracture Risk
Hip fracture prevention operates at two levels — preventing the falls that cause fractures, and reducing the probability that a fall produces a fracture when it occurs.
Preventing the Fall
Every fall prevention intervention reduces hip fracture risk by reducing the falls that could cause one. Bathroom modifications address the highest-risk fall environment. As covered in our guide on the bathroom causes more senior falls than stairs, cars, and ice combined — grab bars at the shower entry and next to the toilet address the two highest-risk daily transitions.
→ Get the 2-Pack Grab Bars on Amazon
Medication review specifically for fall risk — the single most significant modifiable fall risk factor. Balance exercise that reduces fall rates by 30 percent. Vision correction that addresses the visual contribution to balance. Home hazard removal that addresses the environmental risk factors.
Our complete guide on fall prevention for seniors covers every evidence-based intervention in one comprehensive resource.
Reducing Fracture Risk From Falls That Do Occur
Bone density assessment and management directly affects whether a fall produces a fracture. A DEXA scan identifies current bone density and fracture risk. For those with osteopenia or osteoporosis medical management through medication, calcium, vitamin D, and weight-bearing exercise reduces fracture probability from falls that do occur.
Vitamin D specifically is worth discussing with the physician managing care — deficiency is both independently associated with fall risk and with reduced bone density. Assessment and supplementation addresses both simultaneously for anyone with documented deficiency.



What the 50 Percent Means for Independent Living Planning
The 50 percent figure is the most compelling argument available for proactive aging in place planning — because it demonstrates that independent living, once lost to a hip fracture, is not reliably recovered.
This changes how aging in place modifications should be framed. A grab bar at the shower entry isn’t a convenience. It’s the modification that may determine whether a person is living in their own home in five years or in a care facility. A bed rail for the morning getting-up transition isn’t an accommodation. It’s protection for the daily moment most likely to produce the fall that produces the fracture that produces the statistic.
As covered in our guide on what is aging in place — the modifications that support aging in place are most effective when they’re made before they’re urgently needed. The modifications made after a hip fracture address the risk for the next fall. The modifications made before it prevent the fracture that reorganizes the life.


The Detection Gap — What Happens After the Fall
Hip fractures that occur when no one is present — during a solo bathroom trip, during a nighttime getting-up, anywhere in a home where someone lives alone — may not be discovered for hours. As covered in our guide on what happens to seniors who fall and can’t get up — the time on the floor compounds the fracture with additional medical consequences that worsen outcomes.
Automatic fall detection that alerts family immediately when a fall occurs addresses this gap specifically. The SecuLife Smartwatch worn on the wrist detects falls automatically and alerts designated family contacts with real-time GPS location — without any action required from the person who has fallen. For someone who has broken a hip and is on the bathroom floor at 2am it’s the difference between help arriving in minutes and help arriving hours later.
→ Get the SecuLife Smartwatch on Amazon
The Conversation the 50 Percent Statistic Enables
Most families find the fall prevention conversation difficult to have — because it touches on independence, decline, and the future in ways that feel threatening. The 50 percent statistic changes the framing of that conversation.
It’s not a conversation about what might happen. It’s a conversation about what happens to half of older adults who break a hip — and what specifically reduces the probability of being in that half. That’s a different conversation. It’s a planning conversation rather than a fear conversation. A specific conversation rather than an abstract one.
As covered in our guide on how to talk to an aging parent about moving and our guide on your parent said they’re fine — the conversations that work are the ones that treat the parent as a capable person making informed decisions about their own life. The 50 percent statistic is information that capable people deserve to have when making those decisions.

The Other 50 Percent
The statistic also tells us that half of hip fracture patients do return to something close to their pre-fracture life. They’re not lucky. They’re the ones whose fractures were treated promptly. Whose rehabilitation was aggressive and early. Whose nutrition during recovery was monitored and supported. Whose families advocated for orthogeriatric co-management. Whose homes were modified before their return so that recovery happened in a safer environment than the one where the fall occurred.
Outcomes are not fixed. The 50 percent figure is what happens on average across all patients in all circumstances. Specific circumstances produce better outcomes — and knowing what those circumstances are is what allows families to create them.
Our guide on how long seniors live after a fall covers the complete picture of post-fall outcomes — including what specifically improves them. Our guide on how to help an elderly parent after a fall covers the immediate response that changes what the fall becomes.


About the Author
Margaret Holloway, RN spent 22 years in geriatric nursing watching the hip fracture statistic become real individual lives — the patient who came in from their own home and left for a care facility, the family that didn’t know the 50 percent figure until they were living it. She also watched the families who did know — who had modified the home, who had the conversation, who had the fall detection in place — navigate a hip fracture with significantly better outcomes than the population average. The statistic is real. So is the variability around it. And the factors that determine which side of it a person ends up on are specific enough to act on before the fracture makes the question urgent. She writes for Elder Safety Guide because knowing the 50 percent figure before a hip fracture is what allows families to do something about it.